Congratulations to Florin who is the expression of the month contest winner for February. We would categorize this expression as a nice, big, social smile. Florin wins a free online key to a training of his choice and he wisely chose one of our most advanced courses, MiX Elite.

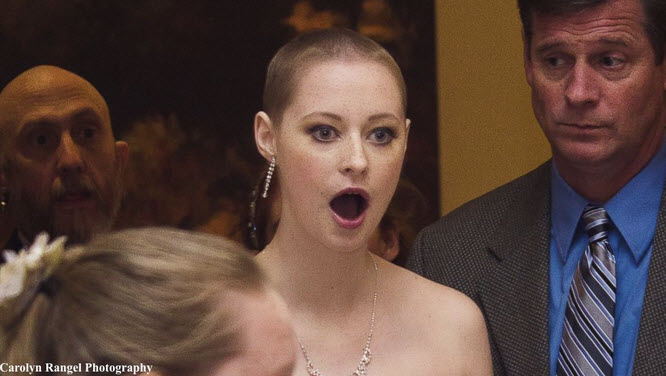
FACS codes are 6B + L7C + 12DE + 25